normal sinus rhythm with one premature supraventricular beat

First Glance:
This is presumably sinus rhythm, based on the regular P waves before all QRS complexes, with normal PR interval and normal (upright) P wave axis in lead II.
Discussion:
We can also see one premature beat late in the strip. We can’t see any P wave before it, so it may be buried in the T wave, or it might come from a junctional source with no associated prior atrial depolarization. We know it is premature because it is clearly early (we would call it an escape beat if it was late). I think it is supraventricular because it is narrow complex, although it is on the wide side of narrow complex- maybe just under 120ms.
While the morphology is similar to the other QRS complexs, the deflection is smaller and it has a terminal S wave that the native beats don’t have. Perhaps this is due to incompletely repolarized ventricular myocardium or conduction fibers resulting in a little aberrancy, or to a superimposed P wave.
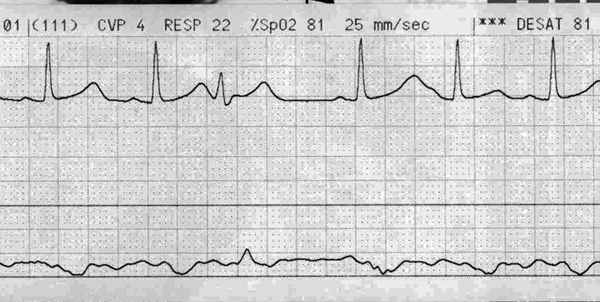
You can see that after the extra beat there is a pause. That pause results in higher ventricular preload for the next beat (more filling time results in higher filling volume and therefore higher filling pressure). This results in a more powerful contraction/depolarization, which may result in the longer and larger T wave in the subsequent beat, which blurs with the next P wave. The system then falls back into its prior rhythm.
If you think I was just making up all that nonsense about the preload then just look at the lower tracing, which is the Central Venous Pressure (CVP). Below you can pick out the A, C, and V waves nicely, with the respective X and Y descents.
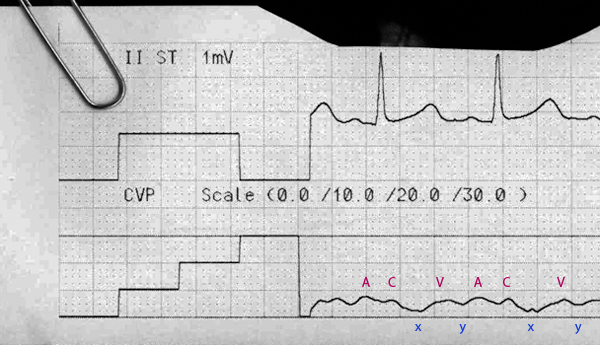
The A wave is the backwash of the right Atrial contraction. The C wave is the backwash from the ventricular Contraction bowing the tricuspid valve into the atrium. The X descent is the relaXation phase of the atria (technically starts before, and is interrupted by, the C wave) and the V wave is the rapid filling of the atrium during diastole. The Y descent is the rapid passive emptying of the atria into the ventricles prior to atrial systole.
Note that the A wave is not directly under the EKG P wave, and the C wave is not directly under the EKG QRS complex. This is because it takes a few milliseconds for the depolarization to be converted into force and then actually start moving fluid.
So what does the CVP tracing tell us about our preload/electrophysiology theory? Look at the CVP through the ectopic beat and subsequent pause.

We can see that the CVP generally falls to near zero after the X descent (relaxation phase of the atria). However, when the premature beat depolarizes the ventricle it looks like there is no Y descent, which suggests that the the atrium never enjoyed its rapid emptying into the ventricle, therefore the CVP never falls to zero. This might suggest a premature junctional beat (without it’s associated prior atrial kick), and the new cycle starts from a higher CVP baseline (orange triangle above) and reaches a slightly higher end-diastolic CVP.
That marked positive spike in the CVP tracing before the orange triangle is probably an A wave (either from a retrograde atrial depolarization, or from an on-time sinus P wave) from an atrial contraction that happened while the tricuspid valve is closed (because we are in the middle of ventricular systole here). Note that the spike coincides exactly with where we would have expected the next sinus P. If the sinus node did not get reset by this premature beat, that is again more consistent with an ectopic beat originates below the atria (ie: junctional or below).
Final Impression?
NSR @ 90 bpm with one premature junctional beat, plus a lot of mental masturbation.
Management implications:
None whatsoever. The rhythm is unremarkable and the CVP is normal. Even if the ectopy gets far more frequent it is unlikely to have any bearing on the cardiac output. It can be a sign of stress, however, as might be seen in adrenergic stimulation, wall stretch due to fluid overload or valvular pathology, etc, so it is not necessarily something to be ignored.
The Take-home Point:
Even from a straightforward strip we can dissect out a lot of interesting cardiac physiology.
![]() One star strip. Students should identify the rhythm.
One star strip. Students should identify the rhythm.